Dominique J. Griffon, DMV, MS, PhD, DACVS, DECVS
Associate Professor, Head, Small Animal Surgery Director, Laboratory for Orthopedic Research on Biomaterials University of Illinois, Small Animal Clinic
Urbana, IL, USA
Cranial cruciate ligament (CCL) rupture is one of the most common injuries to the stifle of dogs and is the leading cause of degenerative joint disease in that joint (Johnson JA et al. 1994, Innes JF et al. 2000, Elkins AD et al. 1991). The annual economic impact of medical and surgical management of CCL insufficiency has recently been estimated to about 1 billion dollars in the United States alone (Wilke et al. 2005). Whereas traumatic rupture of CCL predominates in humans, CCL deficiency in dogs is typically associated with a chronic history of progressive lameness consistent with a degenerative process. Misalignment of the joint surfaces is a well-recognized cause of arthrosis and gait abnormalities. Techniques altering overall limb and specific joint alignment have recently gained popularity to prevent or correct surgical diseases of the joints, including CCL disease.
This presentation will first review the clinical and radiographic measurements used to evaluate alignment of the rear leg in the canine patient, along with potential applications of advanced imaging techniques. Clinical cases will be presented to illustrate abnormalities measured with each technique in dogs with cruciate ligament disease. The changes in joint and limb alignment produced by surgical procedures currently recommended for the treatment of CCL will be described, along with their limitations and potential future modifications.
Rupture of the CCL has been associated with degenerative changes, auto-immune diseases, hormones (sex predisposition), collagenase activity and antibodies against type-I and-II collagen in synovial fluid (Comeford 2003, Moore KW, Read RA 1996). However, weakening secondary to repetitive microtrauma is currently believed to cause the majority of CCL instabilities diagnosed in dogs, especially in large breeds such as Labradors (Hayashi K et al. 2003, Duval JM et al. 1999, Arnoczky SP, Marshall JL 1981). A great deal of interest has recently focused on the importance of the "cranial tibial thrust" as an underlying cause for repetitive microtrauma to the CCL (Slocum B, Devine T 1983). This force generated by compression between the tibia and femur during the stance (weight-bearing) phase, is partly oriented in a cranial direction, leading to cranial translation of the tibia. In a stable knee, this force is actively opposed by the pull of the stifle flexor muscles (Figure 1).
| Figure 1. | 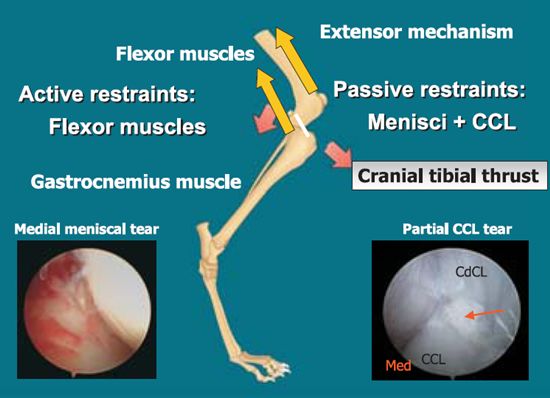
Schematic representation of forces acting at the knee (derived from Slocum B and Devine TD, 1993). Cranial tibial thrust (CTT) is generated by weight bearing and contraction of the gastrocnemius muscle. The extensor mechanism also contributes to compression between the femur and the tibia. CTT is counteracted by the flexor muscles and passive restraints |
|
| |
The magnitude of this force generated by contraction of the gastrocnemius depends on the amplitude of the compressive force (70% of the body weight at trot) but also on the slope of the tibial plateau with respect to the axis joining the centers of motion of the stifle and hock. This theory provides a basis for the Tibial Plateau Leveling Osteotomy (TPLO), a procedure that is not aimed at restoring the anatomical stability of the CCL deficient stifle (Slocum B, Devine TD 1993). Instead, it modifies the joint geometry to neutralize cranial tibial thrust during weight bearing. Although this procedure has gained tremendous popularity for treatment of CCL deficiency in large breed dogs, several studies have failed to show a correlation between the steepness of the tibial plateau and the development of CCL insufficiency (Reif U, Probst CW 2003, Wilke VL et al. 2002).
This reflects the fact that these stress injuries most likely result from a combination of, rather than from a single factor. Indeed, the biomechanical environment leading to CCL instability can be described as an imbalance between factors contributing to the CTT and its active restraints (illustrated in Figure 1), eventually leading to fatigue failure of the passive restraints (CCL and medial meniscus). This model would explain the association between obesity (increasing the compressive force applied on the knee) and CCL deficiency (Duval JM et al. 1999). The proposed biomechanical model could also explain the mechanism of action of conformation abnormalities previously believed to lead to CCL deficiency, such as genu varum, increase in stifle angle (straight-legged dogs such as Labrador Retrievers), tarsal hyperextension, deformation of the proximal tibia or stenosis of the intercondylar notch (Fitch RB et al. 1995, Moore KW, Read RA 1996). Genu varum consists of a varus deformation of the femur, resulting in a "bow-legged" stance. This conformation has been associated with medial patellar luxation (MPL). MPL tends to cause an internal rotation, which is prevented in part by the CCL. Misalignment of the patellar tendon affects the direction of forces generated by the quadriceps and destabilizes the anterior compartment of the knee.
The impact of the thigh muscles on the magnitude of the CCT remains poorly defined. Yet, an imbalance between flexor and extensor muscles of the thigh would contribute to CCL overuse. This imbalance could result from a difference in muscle distribution that could potentially be corrected via physical therapy. Another potential cause of imbalance between muscle groups could result from a cranio-caudal misalignment of the quadriceps, affecting the direction and moment of forces generated during weight bearing. This theory would support the mechanism of action of tibial tuberosity advancement (TTA) as a recently proposed treatment for CCL deficiency. This procedure maintains the angle between the patellar tendon and the tibial plateau to a maximum of 90° in full extension, thereby loading the caudal cruciate ligament throughout the entire range of motion of the knee (Tepic S, 2004). TTA involves a pre-determined open wedge osteotomy of the tibial tuberosity that is fixed with a tension band plate and grafted.
Proximal tibial shaft deformity was recently described in 9% of dogs with CCL and steep tibial plateau slope (Osmond et al. 2006). The deformity consisted of a caudal tipping (greater than 11°) of the proximal tibia in relationship with its long axis, thereby identifying a distinct subpopulation of dogs with CCL disease. Although these findings warrant further investigation, they may eventually affect our therapeutic recommendations. Indeed, a cranial tibial wedge would re-align the entire proximal tibia, and may therefore be a better option than TPLO in these dogs.
The multifactorial origin of CCL deficiency secondary to repetitive microtrauma most likely involves the tibial plateau slope along with other morphometric parameters, whose relative contributions have yet to be defined. Variations between breeds, difficulties identifying "normal" versus "predisposed" dogs, invasiveness and cost of procedures hinder our ability to design meaningful studies and improve our understanding of the pathogenesis of CCL disease. Studies evaluating the potential contribution of conformation characteristics to CCL injuries have largely been based on clinical and radiographic assessments (Wilke VL et al. 2002, Duval JM et al. 1999, Aiken SW et al. 1995, Whitehair JG et al. 1993). The conformation of the entire limb in dogs predisposed to CCL deficiency has not been systematically evaluated. Computerized tomography has been applied to study the musculature of the thigh and lower extremity in humans with ACL injuries (Lorentzon R et al. 1989, Gerber C et al. 1985). This non-invasive imaging technique has also been used to estimate body segment parameters (such as length, mass and location of the center of mass) in living subjects. These morphometric parameters have then been combined with kinetic and kinematic data to calculate moment of forces and mechanical power at a joint, applying inverse dynamic analysis of gait. This approach to biomechanical gait analysis has greatly contributed to the understanding of mechanisms of orthopedic disorders such as ACL injuries in humans (Decker MJ et al. 2003, Chappell JD et al. 2002). We are currently applying this technique to Labradors with and without CCL insufficiency to try and identify conformation factors that predispose this breed to the disease. The long term goal of this research is to allow the development of preventive measures, such as physical therapy to correct muscle imbalance and/or alteration of growth plate(s) to modify skeletal growth and conformation.
References
1. Aiken SW, Kass PH, JP Toombs: Intercondylar notch width in dogs with and without cranial cruciate ligament injuries. Vet Comp Orthop Traumatol 1995 8: 128-132.
2. Arnoczky SP, Marshall JL: Pathomechanics of cruciate and meniscal injuries. In Bojrab MJ (ed): Pathophysioloy in Small Animal Surgery. Lea & Febiger, Philadelphia 1981, p 590.
3. Chappell JD, Yu B, Kirkendall DT et al.: A comparison of knee kinetics between male and female recreational athletes in stop-jump tasks. American J Sports 2002; 30: 261-267.
4. Comeford E: Comparison of biochemical and biomechanical properties of cranial cruciate ligament in the Greyhounds, Labrador Retriever and Golden Retriever. PhD thesis, Department of Clinical Veterinary Science, University of Bristol, 2003.
5. Conzemius M, Robinson D, Evans R et al.: Estimate of the annual economic impact of rupture of the cranial cruciate ligament in the dog in the United States. Proc scientific meeting of the Veterinary Orthopedic Society, Big Sky, Montana, February 21-28, 2004, pp 44.
6. Decker MJ, Torry MR, Wyland DJ et al.: Gender differences in lower extremity kinematics, kinetics, and energy absorption during landing. Clinical Biomechanics 2003; 18: 662-669.
7. Duval JM, Budsberg SC, Flo GL et al.: Breed, sex and body weight as risk factors for rupture of the cranial cruciate ligament in young dogs. J Am Vet Med Assoc 1999; 215: 811-814.
8. Elkins AD, Pechman R, Kearney MT, et al.: A retrospective study evaluating the degree of degenerative joint disease in the stifle of dogs following surgical repair of anterior cruciate ligament rupture. J Am Anim Hosp Assoc 1991: 27: 533-540.
9. Fitch RB, Montgomery RD, Kincaid SA et al.: The effect of intercondylar notchplasty on the normal stifle. Vet Surg 1995; 24: 156-164.
10. Gerber C, Hoppeler H, Claassen H et al.: The lower-extremity musculature in chronic symptomatic instability of the anterior cruciate ligament. J Bone Joint Surg Am 1985; 67: 1034-1043.
11. Hayashi K, Frank JD, Dubinsky C et al: Histologic changes in ruptured canine cranial cruciate ligament. Vet Surg 2003; 32: 269-277.
12. Innes JF, Bacon D, Lynch C et al.: Long-term outcome of surgery for dogs with cranial cruciate ligament deficiency. Vet Rec 2000; 147: 325-328.
13. Johnson JA, Austin C, Breur GJ: Incidence of canine appendicular musculoskeletal disorders in 16 veterinary teaching hospitals from 1980 to 1989. Vet Comp Orthop Traumatol 1994; 7: 56-59.
14. Lorentzon R, Elmqvist LG, Sjostrom M et al.: Thigh musculature in relation to chronic anterior cruciate ligament tear: muscle size, morphology, and mechanical output before reconstruction. Am J Sports Med 1989; 17: 423-429.
15. Moore KW, Read RA: Rupture of the cranial cruciate ligament in dogs--Part I. Comp Cont Ed Pract 1996; 18: 223-234.
16. Osmond CS, Marcellin-Little DJ, Harrysson OL et al.: Morphometric assessment of the proximal portion of the tibia in dogs with and without cranial cruciate ligament rupture. Vet Radiol Ultrasound, 2006; 47: 136-141.
17. Reif U, Probst CW: Comparison of tibial plateau angles in normal and cranial cruciate deficient stifles of Labrador Retrievers. Vet Surg 2003; 32: 385-389.
18. Slocum B, Devine TD: Tibial plateau leveling osteotomy for repair of cruciate ligament rupture in the canine. Vet Clin North Am Small Anim Pract 1993; 23: 777-795.
19. Slocum B, Devine T: Cranial tibial thrust: a primary force in the canine stifle. J Am Vet Med Assoc 1983; 183: 456-459.
20. Tepic S, Montavon PM: Is cranial tibial advancement relevant in the cruciate deficient stifle? Proc. 12th ESVOT congress, Munich, 2004: 132-133.
21. Whitehair JG, Vasseur PB, Willits NH: Epidemiology of cranial cruciate ligament rupture in dogs. J Am Vet Med Assoc 1993; 203: 1016-1019.
22. Wilke VL, Robinson DA, Evans RB et al.: Estimate of the annual economic impact of treatment of cranial cruciate ligament injury in dogs in the United States. J Am Vet Med Assoc 2005; 227: 1604-1607.
23. Wilke VL, Conzemius MG, Besancon MF et al.: Comparison of tibial plateau angle between clinically normal Greyhounds and Labrador Retrievers with and without rupture of the cranial cruciate ligament. J Am Vet Med Assoc 2002; 221: 1426-1429.